
5.2 Entropion
Introductory Comments
Candidates should direct their examination towards determining the:
- Cause of the entropion
- Potential surgical options to address the entropion
- The presence of corneal complications such as ulceration or scarring
This is relevant for determining severity of keratopathy as well as the viability of certain surgical repair options (such as prolonged surgical closure of the lids).
Stand back from the patient and observe for a few seconds, then advance closer and continue to observe. While observing comment on the features mentioned below:
- Entropion (may be brought out by forced lid closure / supine posture)
- In-turned eyelashes (not true trichiasis if the eyelashes sit properly when lid is everted)
- Conjunctival injection, epiphora
- Shortened inferior fornix or symblepharon suggests a cicatricial component
- Superior override of the preseptal orbicularis noted with forced closure of the eyelid
Pull the lower lid down and ask the patient to look up. Observe the inferior fornix. Then ask the patient to look down. Observe the tarsal plate and fornix for movement.
- A tarsal entropion (frank inversion of the tarsal plate) indicates dehiscence or severe attenuation of the inferior retractors and their insertion to the lower tarsal plate. In less severe ectropion the presence of retractor dehiscence is suggested by:
- Deepening of the inferior fornix
- Visible separation of retractors from the tarsal plate (a red area between the white band of the retractors and the inferior tarsus)
- Lack of movement of the distracted lower lid with downgaze
Generalised Lid Laxity
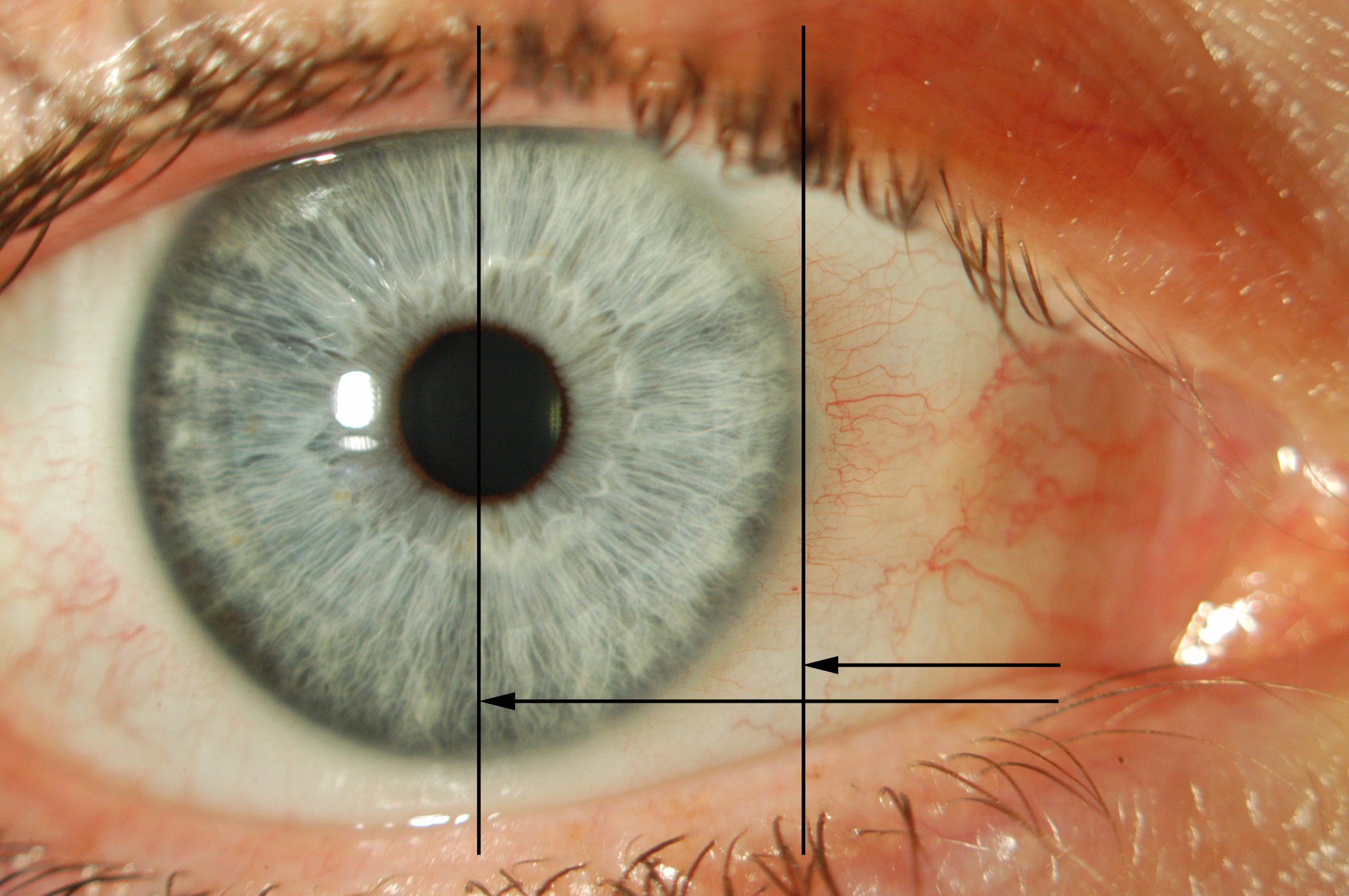
Distraction and “Snap back” test: Pull the lower lid directly away from the globe and observe how far it can be distracted (> 8 - 9mm is considered “abnormal”) and how quickly it “snaps back” onto the globe when released. A normal eyelid does not require a blink to reposition itself on the globe
Lateral Canthal Tendon (LCT) Laxity
Note any rounding of the lateral canthus. Pinch the lower eyelid and pull medially (“Medial distraction test”). Medial distraction of the lateral canthus > 2mm is abnormal. Compare with the contralateral side
Medial Canthal Tendon (MCT) Laxity [i]
Note the resting position of the punctum. Pinch the lower eyelid and pull laterally (“Lateral distraction test”)
- “Moderate”: Punctum reaches limbus
- “Severe”: Punctum reaches pupil – (stabilisation of the MCT may be required)
There is no universally agreed grading system for MCT laxity. Readers are encouraged to refer to Olver et. al. Lower Eyelid Medial Canthal Tendon Laxity Grading. Ophthalmology. 2001 Dec;108(12):2321-5.
This completes the examination that has been done up to this point. Look for:
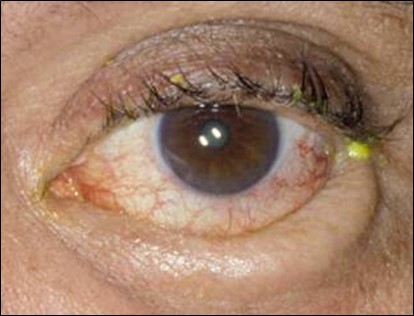
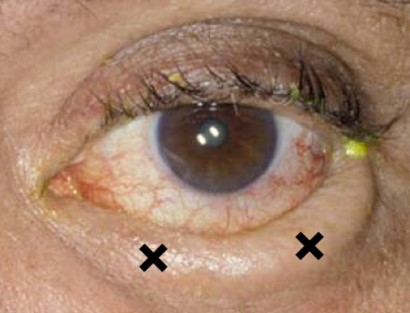
- Fluorescein staining: Punctate epithelial erosions or epithelial defect
- Corneal scarring (from chronic irritation)
- Conjunctival inflammation, symblepharon, shortened inferior fornix
- Suspicious skin, lid margin or conjunctival lesions (exclude malignancy)
The pathogenesis of entropion is very similar to that of ectropion- i.e. horizontal lid laxity and inferior retractor instability (± cicatricial components). Various theories have been proposed but it is not known exactly why some people develop ectropion and others entropion as differing sequelae to similar involutional processes.
Congenital
Rare
Acquired
- Involutional
a. Orbicularis: Pre-septal over-rides pre-tarsal muscle
b. Retractor laxity
c. Tarsal plate laxity
d. Horizontal lid laxity (MCT & LCT) - Cicatricial
a. OCP
b. Chemical burn
c. Stevens-Johnson syndrome
d. Trachoma
e. Chronic blepharitis
f. Prolonged topical drop usage (e.g. glaucoma) - Acute spastic
a. Ocular irritation / inflammation → Orbicularis contraction
Depends on:
- Type
- Severity
- Extent
Most cases of entropion will require definitive surgical treatment. Cases of entropion which are constant (not intermittent) and not controlled by conservative measures should be repaired as promptly as possible due to the risk of corneal infection or scarring from lashes rubbing on the cornea.
1. Conservative
- Taping eyelid, lubricants
- Spastic element: may improve with resolution of acute problem (e.g. conjunctivitis)
2. Botulinum Toxin
Localised pharmacological paralysis of the pre-tarsal orbicularis can prevent the overriding and temporarily resolve the entropion. The effect is variable in duration and efficacy and will not work in a purely cicatricial ectropion. Administer 5 units of Botox® (Allergan, Dublin, Ireland) (or equivalent dose of other botulinum toxin) in 0.1mL to the medial and lateral pre-tarsal orbicularis muscle as an initial dose (see Figure 5.2.3 below).
Previous
5.1 Ectropion
Next
5.3 Eyelid Tumours
All rights reserved. No part of this publication which includes all images and diagrams may be reproduced, distributed, or transmitted in any form or by any means, including photocopying, recording, or other electronic or mechanical methods, without the prior written permission of the authors, except in the case of brief quotations embodied in critical reviews and certain other noncommercial uses permitted by copyright law.

Vitreoretinal Surgery Online
This open-source textbook provides step-by-step instructions for the full spectrum of vitreoretinal surgical procedures. An international collaboration from over 90 authors worldwide, this text is rich in high quality videos and illustrations.