
8.2 Subjective Refraction
1. Measure the Visual Acuity with the Retinoscopic Prescription
- Begin by occluding the opposite eye.
- If the VA is 6 / 6… only very small adjustments will be required
- If the VA is 6 / 9 or worse… larger adjustments will be required
- As a rough guide a 0.25D change in refraction should lead to a one Snellen line improvement
2. Check the Sphere (Avoid “Over-Minusing”)
- In pre-presbyopic patients, unless the patient is cyclopleged, active accommodation can result in a prescription that is “over-minused” (or too myopic) as their active accommodation absorbs additional minus. Therefore, the goal of the subjective refraction is to find the maximum plus (or minimum minus) that provides the maximum acuity (i.e. if additional minus is not improving visual acuity and just making the letters smaller and darker rather than clearer, it is not required)
A. If the Patient is >60 Years or Pseudophakic:
- Add plus / minus spheres (as accommodation is not an issue) to maximise visual acuity, asking “Do you prefer lens 1 or 2” etc
B. If the Patient is <60 Years (Consider That They May be Pre-presbyopic):
- Add + 0.5D
- Ask “Does this make your vision worse?” (adding plus to blur the patient is referred to as “fogging”)
- “No” → Add the + 0.5D and repeat
- “Yes” → Add - 0.25D, Ask “Does this make your vision better?”
- “No” → The sphere is already correct
- “Yes” → Add the -0.25D and repeat
Notes:
- In a pre-presbyope, adding the - 0.25D won’t usually make their vision worse since the patient can accommodate to bring the image forward onto the retina. When changing plus lenses, always keep a plus lens over the eye (“protect the fog” by placing the new plus lens before removing the old plus lens) to ensure that the patient doesn’t accommodate
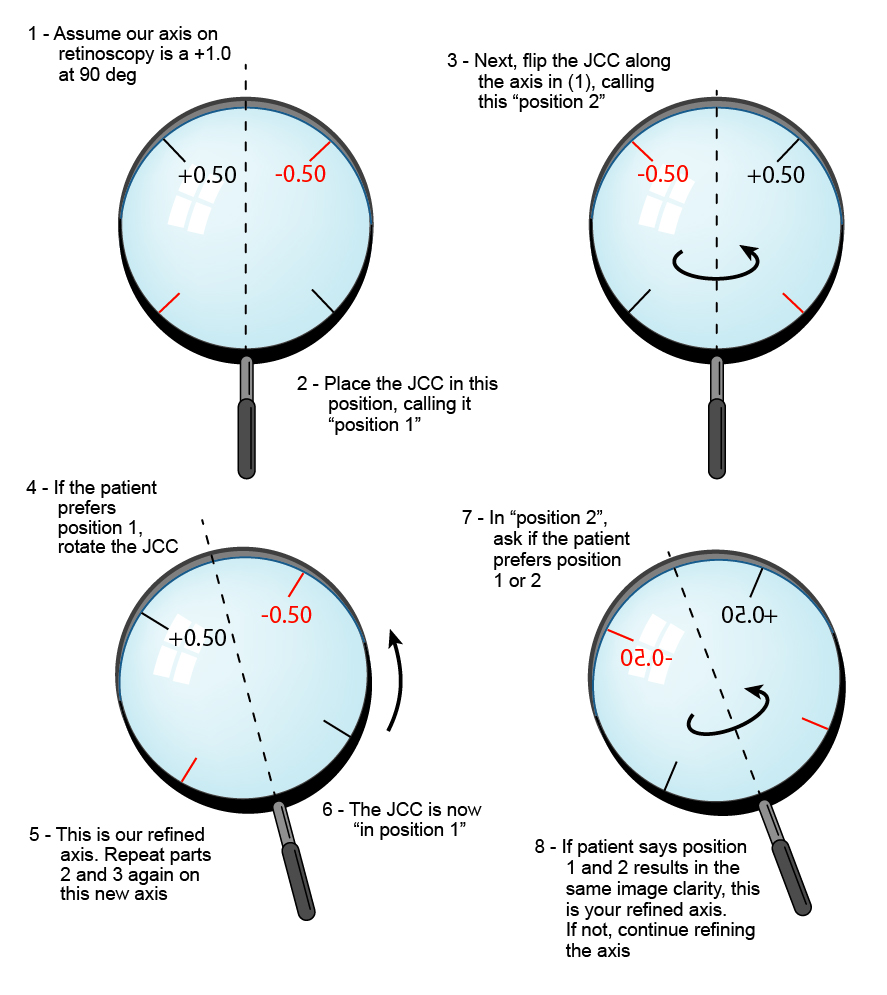
3. Refine the AXIS of the Cylinder
- Always refine the cylinder axis before the power (because the correct axis can be found in the presence of incorrect power, but the correct power cannot be found in the presence of an incorrect axis). Higher powered Jackson Cross Cylinders (JCCs) are used for axis determination; lower powered JCCs are used for power refinement
- Ask the patient to look at a round target (e.g. “O”) ~two lines above the maximum acuity read with the best sphere
- Align the handle of the Jackson cross cylinder along the axis of the cylindrical lens in the trial frame
- Flip the Jackson cross cylinder, telling the patient “These may both make it worse, but tell me which is the clearer of the two “1”… or "2”?” When flipping the Jackson cross cylinder, pause to give the patient sufficient time to appreciate each orientation, but make the “flips” sharp and quick
- After determining the orientation of the JCC that the patient prefers, rotate the cylinder in the trial frame towards the side of the same cylinder sign on the JCC (e.g. plus cylinder to plus cylinder on JCC). If the cylinder power is not high, rotations should initially be in ~15° steps, then reduced as the correct axis is approached. Be sure to re-align the handle of the JCC to the new axis before you re-test
- Continue until both orientations look the same to the patient, or you are switching between a narrow range of axes (in this case select the middle of the range)
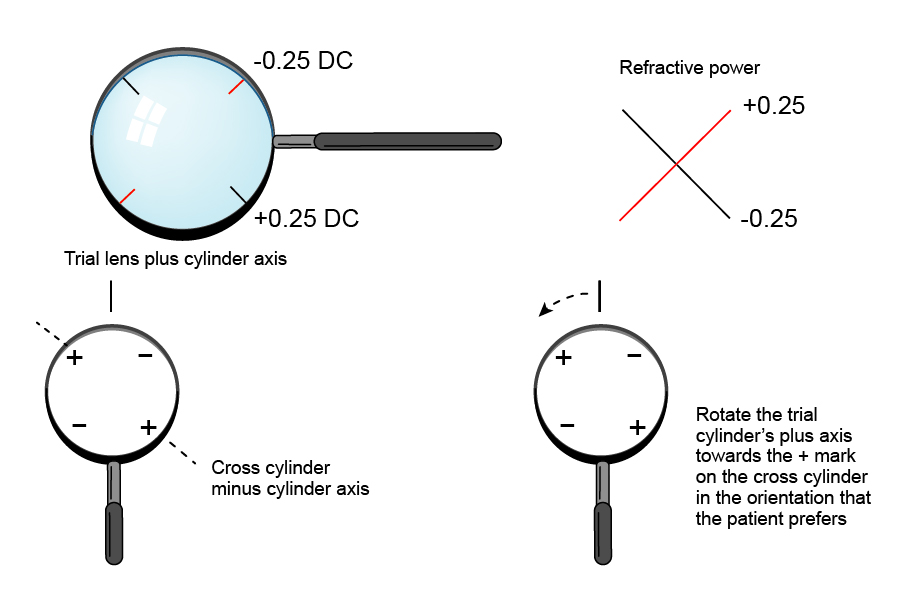
4. Refine the POWER of the Cylinder
- Align one axis of the Jackson cross cylinder along the axis of the cylindrical lens in the trial frame.
- Flip the Jackson cross cylinder slowly, asking the patient “Tell me which is the clearer of the two “1”… or “2”?” When flipping the Jackson cross cylinder, pause to give the patient sufficient time to appreciate each orientation, but make the “flips” sharp and quick
- If the patient finds it clearer when the “+” sign on Jackson cross cylinder is in line with cylinder axis, add + 0.25D. If the patient finds it clearer when the “-“ sign on Jackson cross cylinder is in line with cylinder axis, add - 0.25D.
- Continue until both orientations look the same to the patient
5. Refine the Sphere Again
- For each 0.50D increase in cylinder power, - 0.25D will need to be added to sphere to maintain the position of the circle of least confusion. Similarly for every 0.50D reduction in plus cylinder, + 0.25D will need to be added to the sphere. The target is the most plus, or least minus sphere that yields maximum visual acuity (since you don’t want to overcorrect myopes, making them accommodate thus causing eye strain)
Duochrome
- Check this by ensuring that the patient is slightly on the red side of the duochrome visual acuity chart (“RAM-GAP”: “red add minus, green and plus”)
- (In other words, do NOT over minus a patient!)
6. Near Vision
- Assess the patient’s need for a near correction (i.e. presbyopes). The power of the near add will be determined by their daily activities and how close they normally hold near objects for viewing
Pinch to zoom
Figure 8.2.3
Using the Jackson Cross Cylinder to Determine the Cylinder Axis
Hold the JCC so that the handle aligns along the axis of the cylindrical lens in the trial frame. Flip the cross cylinder and determine which orientation the patient prefers. Rotate the cylinder in the trial frame towards the side of the same cylinder sign on the JCC. Repeat until the patient does not have a preference for one orientation.
All rights reserved. No part of this publication which includes all images and diagrams may be reproduced, distributed, or transmitted in any form or by any means, including photocopying, recording, or other electronic or mechanical methods, without the prior written permission of the authors, except in the case of brief quotations embodied in critical reviews and certain other noncommercial uses permitted by copyright law.

Vitreoretinal Surgery Online
This open-source textbook provides step-by-step instructions for the full spectrum of vitreoretinal surgical procedures. An international collaboration from over 90 authors worldwide, this text is rich in high quality videos and illustrations.