
7 Neuro-Ophthalmology
7.1 Cranial Nerve III (Oculomotor) Palsy
7.2 Cranial Nerve IV (Trochlear) Palsy
7.3 Cranial Nerve VI (Abducens) Palsy
7.4 Cranial Nerve VII (Facial) Palsy
7.5 Optic Nerve Function
7.6 Visual Fields to Confrontation
7.7 Pupils
7.8 Horner’s Syndrome
7.9 Nystagmus
7.10 Neuro-Ophthalmic Differential Diagnoses and Aetiologies
7.4 Cranial Nerve VII (Facial) Palsy
Cranial Nerve VII palsies may require the candidate to determine:
1. The location of the neurological lesion, and exclude life-threatening causes
2. The oculoplastic management to a multi-factorial problem
- Facial asymmetry
- Loss of forehead wrinkles (lower motor neurone CNVII palsy)
- Brow ptosis (not blepharoptosis) / Lid retraction & Superior sclera [iii]
- ↓ Blink “Please blink” Twitch of mouth = aberrant regeneration
- Ectropion (paralytic) / Inferior scleral show / Red eye
- Loss of nasolabial fold
- Drooping angle of the mouth
- Scars / masses (behind ear, parotid, lymphadenopathy)
- Esotropia (CNVI
Check MRD1 if considering a gold weight
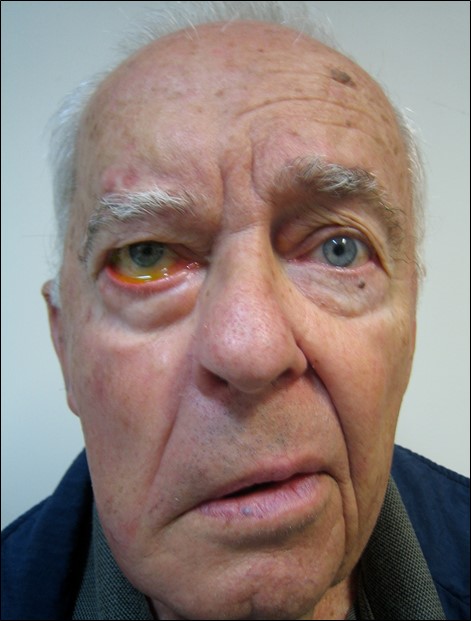
Figure 7.4.1
Right Lower Motor Neurone CNVII Palsy
Note the loss of forehead wrinkles (hence LMN palsy), brow ptosis, paralytic ectropion and less prominent nasolabial fold.
Branch
Instruction to Patient
Examiner Task
i. Temporal
Instruction to Patient
“Look up”
Examiner Task
Try to push down
ii. Zygomatic + Bells
Instruction to Patient
“Close your eyes as tight as you can”
Examiner Task
Try to open
iii. Buccal
Instruction to Patient
“Puff out your cheeks”
Examiner Task
Push in
iv. Mandibular
Instruction to Patient
“Grin like a gorilla / Show me your teeth”
Examiner Task
Narrow inter-palpebral fissure = aberrant regeneration
v. Cervical (platysma)
Instruction to Patient
“Stretch your neck as if shaving”
Examiner Task
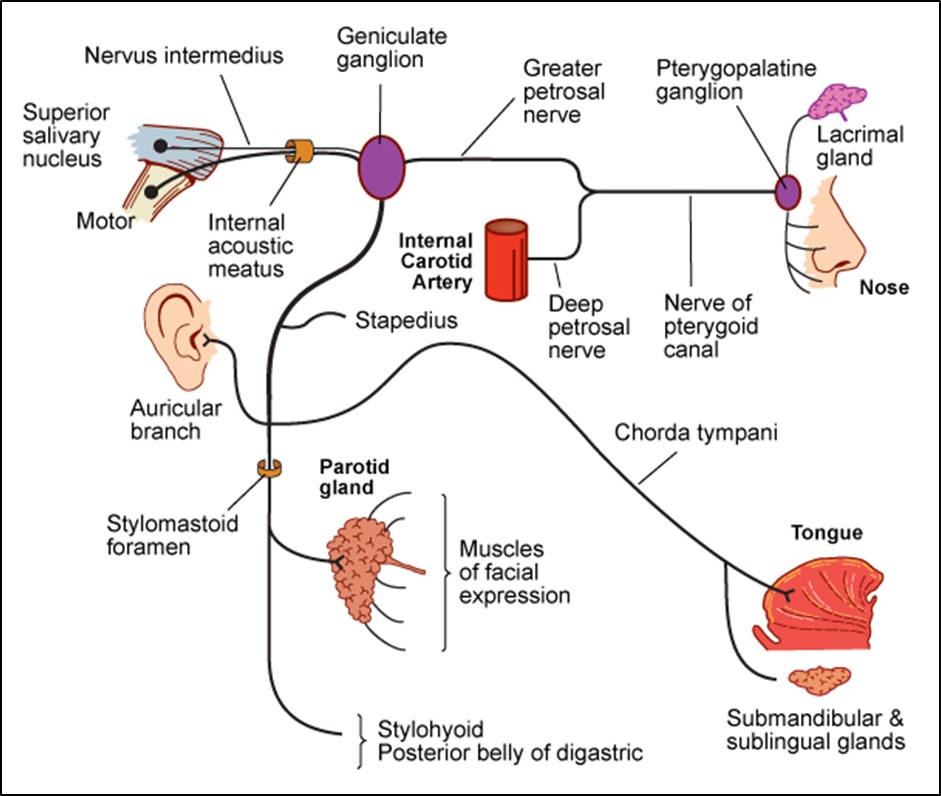
Crocodile tears [iv] = aberrant regeneration
The fibres that originally innervated the submandibular / sublingual glands now innervate the lacrimal gland via the greater petrosal nerve
i. Bells Phenomenon
- Firmly but gently grip both upper eyelids with your thumbs to prevent closing. Ask the patient to “Close your eyes”. With an upward Bells phenomenon, the globes rotate up and out
ii. Lagophthalmos
(2° to upper lid orbicularis dysfunction, unopposed levator)
- Ask the patient to “Rest your head back and gently close your eyes as if you are going to sleep”. Assess whether there is an opening between the upper and lower eyelids- if so, measure this with a ruler
iii. Facial / Corneal Sensation (CN V)
- Ask the examiner for corneal sensation - under examination conditions you will usually be told the result
iv. Dry Eye and Corneal Exposure
- Stain the tear film with fluorescein and examine with a slit lamp for punctate stain
- Check abduction
Test hearing (use 512 Hz tuning fork):
- Hyperacusis = loss of dampening function of stapedius
- Deafness = consider CPA tumour
Check the ears:
- Vesicles in external auditory canal = Ramsay-Hunt
- SCC behind ear = infiltrate facial nerve
- Palpate for tumours
- Check regional lymph nodes
- Corneal exposure?
- Papilloedema?
- Strength
- Cerebellar function – finger-nose
Summary
- Unilateral or bilateral
- Upper vs. lower motor neuron
- Aberrant regeneration
- Corneal exposure (Paralytic ectropion? Neurotrophic cornea?)
- CNVI / VIII involvement
- Ramsay-Hunt
Upper versus Lower Motor Neurone CNVII Palsies
- Upper Motor Neurone (e.g. CVA)
- Spastic paralysis of contralateral lower face
- (Sparing of frontalis & some orbicularis- bilateral innervation)
- Can raise eyebrows
- Lower Motor Neurone (e.g. Bells palsy)
- Flaccid paralysis of ipsilateral side of face
- Can’t raise eyebrow on affected side
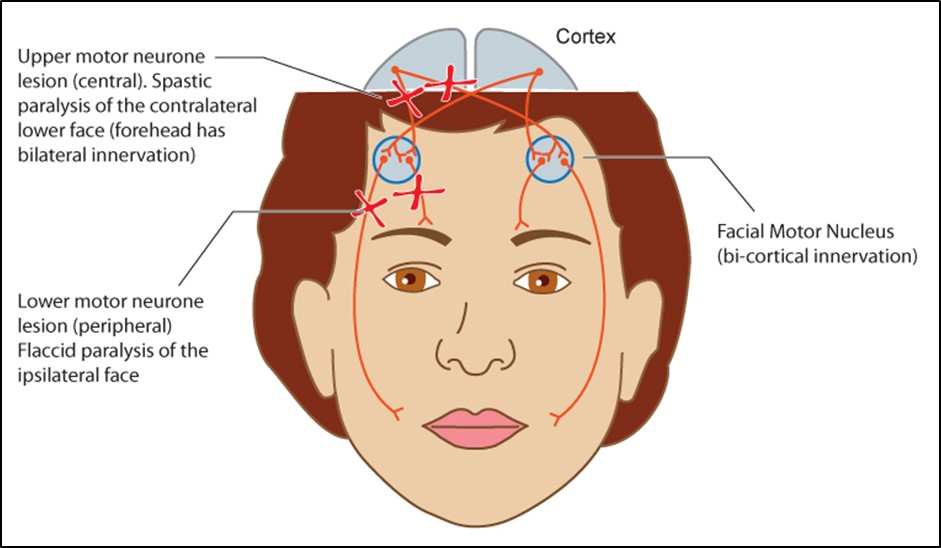
Figure 7.4.3
Upper versus Lower Motor Neurone CNVII Palsies
Upper Motor Neurone lesions produce spastic paralysis of the contralateral lower face. The forehead is unaffected because this has bi-cortical innervation.
Lower Motor Neurone lesions produce flaccid paralysis of the ipsilateral side of the face
- Bell’s palsy is a diagnosis of exclusion and may be related to viral infection (e.g. HSV)
- ⅔ of unilateral CNVII palsy
- Develops over hours
- Unilateral mastoid pain is often present
- 85% get satisfactory recovery by 3 months
- Consider MRI if no improvement
- e.g. parotid
- Ramsay-Hunt syndrome (VZV) – external acoustic meatus (EAM) vesicles, deafness, vertigo
- Chronic otitis media
- Chronic meningitis (TB, Sarcoidosis)
- HIV
- MS
- Guillain- Barré syndrome
- Cerebellopontine Angle CPA (acoustic neuroma, nasopharyngeal cancer, cholesteatoma)
- Parotid Cancer
- SCC with perineural spread
- Diabetes
- Paget’s disease
- Myaesthenia gravis / Guillain-Barré
- Sarcoidosis
- NF-2 (bilateral acoustic neuromas)
- Mobius syndrome
- Basilar meningitis
i. Upper Motor Neurone
- CVA
- Tumour
- Infection
- Demyelination (MS)
ii. Lower Motor Neurone
Brainstem (Pons)
Causes
- CVA
- Tumour
- Infection
- Demyelination (e.g. MS)
Associated Features
- CN V palsy (↓ Corneal sensation)
- CN VI palsy (Diplopia)
- Long-tract signs
All rights reserved. No part of this publication which includes all images and diagrams may be reproduced, distributed, or transmitted in any form or by any means, including photocopying, recording, or other electronic or mechanical methods, without the prior written permission of the authors, except in the case of brief quotations embodied in critical reviews and certain other noncommercial uses permitted by copyright law.

Vitreoretinal Surgery Online
This open-source textbook provides step-by-step instructions for the full spectrum of vitreoretinal surgical procedures. An international collaboration from over 90 authors worldwide, this text is rich in high quality videos and illustrations.