
9 Investigations
9.1 Corneal Topography and Tomography
9.2 Confocal Microscopy
9.3 Optical Coherence Tomography - Macula
9.4 Optical Coherence Tomography Angiography (OCT-A)
9.5 Optical Coherence Tomography - Glaucoma
9.6 Optical Coherence Tomography – Anterior Segment
9.7 Fundus Autofluorescence Imaging
9.8 Fundus Angiography - Fluorescein
9.9 Fundus Angiography - Indocyanine Green
9.10 B-scan Ultrasonography & UBM
9.11 Electrophysiology
9.12 Automated Visual Fields
9.13 Neuroimaging
9.1 Corneal Topography and Tomography
Corneal topography and tomography are often presented as a data station in examinations. Candidates should be able to systematically interpret a scan, and diagnose common conditions in conjunction with clinical findings. Typical cases presented in exams include: keratoconus, pellucid marginal degeneration, post-keratorefractive surgery and post-corneal grafting.
- Ectasias such as keratoconus, pellucid marginal degeneration and post-LASIK ectasia.
- This may be secondary to:
- Corneal grafting
- Refractive surgery complications (e.g. de-centred excimer laser ablation)
- Trauma
- Corneal power measurements for biometry (e.g. post-keratorefractive surgery, for irregular corneas, and for toric intra-ocular lens implantation)
- Prior to keratorefractive surgery (screening for forme fruste keratoconus and other ectasias; planning topography-guided custom ablation)
Corneal topography maps the shape and features of the anterior corneal surface. Corneal topographers analyse the pattern of light rays reflected off the cornea and tear film-air interface and reconstruct the corneal shape. It assumes a fixed relationship between the anterior and posterior curvatures to determine the corneal power.
Corneal tomography evaluates the whole cornea by obtaining information from both anterior and posterior surfaces and evaluates the matter in between. Corneal tomographers are able to reconstruct three-dimensional images of the anterior segment. It gives better estimations of corneal power in patients with irregular corneal astigmatism.
- The reflection off the cornea from multiple concentric rings are analysed to calculate the corneal curvature. Smaller gaps between ring reflections represent steeper curvature; larger gaps represent flatter curvature. Corneal power and elevation are derived from curvature data. Pachymetry is not possible with a pure placido-based system
- Combines placido system for anterior curvature with optical slit system for corneal thickness and elevation data (anterior and posterior corneal surfaces). The slit system captures 240 data points from 40 slits at 45° through the cornea
- Images the anterior segment to the posterior lens surface by using a rotating slit. 50 slit images capture 25,000 true elevation points. Elevation and pachymetric scans are more accurate than with the Orbscan® IIz system, particularly following keratorefractive surgery. The software Belin / Ambrosio Enhanced Ectasia Display uses an “enhanced” best fit sphere and may have improved ability to detect corneal ectasias
- Uses dual Scheimpflug imaging to compensate for decentration / misalignment, combined with placido-based curvature data
- Combines Placido-based Atlas™ topography with OCT pachymetry
- Is prolate (steeper in the centre, flatter in the periphery)
- Has an average:
- Corneal power (K) of ~ 43D
- Central corneal thickness of ~500-550µm
- Posterior float of < +30μm (Orbscan® IIz); < +15µm (Pentacam)
- Is approximately a mirror image of the contralateral cornea
- First confirm the layout and type of the maps presented (this is not standardised). Examine the four maps systematically in sequence, determining if the map is normal, suspicious or abnormal before proceeding to the next
1. Keratometric
- Corneal dioptric power (K). This is more commonly axial than tangential. Note the magnitude and axis of any astigmatism. This should be classified as regular or irregular (further classified as asymmetric, non-orthogonal, or both- see below)
2. Corneal Thickness (Pachymetry)
- Check both central corneal thickness (CCT) on map and “Thinnest” point on data
- Check both the central corneal thickness (CCT) on the map, and the value and position of the “Thinnest” point on the data. Paracentral thinning is suspicious for keratoconus; inferior thinning is suggestive of pellucid marginal degeneration. Thick pachymetry values (> 650μm) may indicate a corneal graft (look for evidence of a graft-host junction), or endothelial failure
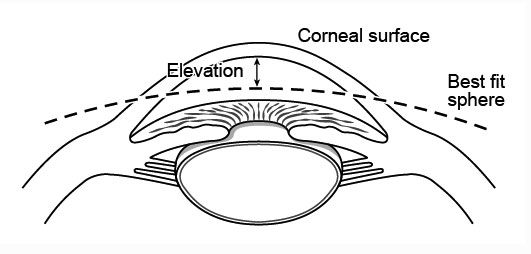
Elevation Maps (Floats)
- These maps display height (not a gradient) of a corneal surface in relation to an arbitrary reference surface (usually a best-fit sphere). Positive values denote height anterior to the reference surface
3. Posterior Elevation (Float)
- Elevation of the posterior corneal surface in relation to a reference surface (usually a best-fit sphere). This may be increased in corneal ectasias (> 20 microns on pentacam or > 40 microns on orbscan is suspicious for ectasia)
4. Anterior Elevation (Float)
- Elevation of the posterior corneal surface in relation to a reference surface (usually a best-fit sphere).
1. Clinical Correlation
- Like all investigations, corneal topography must be interpreted in conjunction with clinical findings.
2. Colours
- Warm colours
- Steep curvature, high power, high elevation, thin pachymetry.
- Cool colours
- Flat curvature, low power, low/depressed elevation, thick pachymetry
- But always check the scales and do not rely on colours alone for interpretation
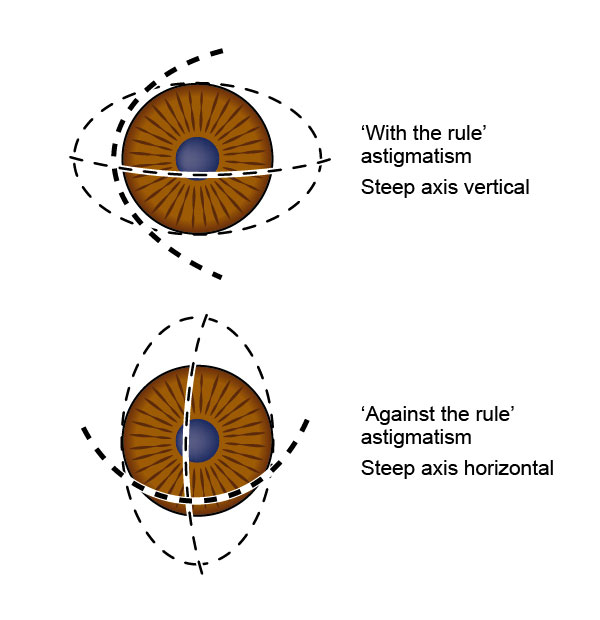
3. Astigmatism
Regular
- Principal meridia are oriented perpendicular to each other
“With the Rule”
- Steep axis closest to vertical (like a football resting on its side)
- E.g. most Keratoconus
“Against the Rule”
- Steep axis closest to horizontal (like a football standing on its point)
- E.g. most Pellucid Marginal Degeneration
Irregular
- Principal meridia are not perpendicular to each other
- Non-orthogonal: Radial arms of steep axis are not in-line
- Asymmetrical: Power of steep axis differs either side of centre
4. Sources of Error
i. Eye
- Misalignment, movement, tear film irregularities, recent contact lens use and ptosis can all introduce potential errors in interpretation
ii. Following Keratorefractive Surgery
- Beware of interpreting elevation and pachymetric scans (particularly Orbscan® IIz) following keratorefractive surgery. The Pentacam is preferable in this situation
iii. Best-fit Sphere
- Note that the best-fit sphere is calculated separately from each elevation map, and this should be taken into account when comparing a series of elevation maps over time
5. Keratoconus
i. Increased Corneal Power
- Paracentral (especially inferotemporal) steepening (high K’s, central > ~ 47D)
- Irregular astigmatism
- Non-orthogonal: radial arms of steep axis subtend an angle > ~ 22°
- Asymmetrical: inferior (higher) - superior (lower) K > ~ 1.5D
ii. Inferior Paracentral Thinning
Previous
8.3 Prescribing Spectacles
All rights reserved. No part of this publication which includes all images and diagrams may be reproduced, distributed, or transmitted in any form or by any means, including photocopying, recording, or other electronic or mechanical methods, without the prior written permission of the authors, except in the case of brief quotations embodied in critical reviews and certain other noncommercial uses permitted by copyright law.

Vitreoretinal Surgery Online
This open-source textbook provides step-by-step instructions for the full spectrum of vitreoretinal surgical procedures. An international collaboration from over 90 authors worldwide, this text is rich in high quality videos and illustrations.