
7 Neuro-Ophthalmology
7.1 Cranial Nerve III (Oculomotor) Palsy
7.2 Cranial Nerve IV (Trochlear) Palsy
7.3 Cranial Nerve VI (Abducens) Palsy
7.4 Cranial Nerve VII (Facial) Palsy
7.5 Optic Nerve Function
7.6 Visual Fields to Confrontation
7.7 Pupils
7.8 Horner’s Syndrome
7.9 Nystagmus
7.10 Neuro-Ophthalmic Differential Diagnoses and Aetiologies
7.2 Cranial Nerve IV (Trochlear) Palsy
Cranial nerve IV palsies are extremely common in examinations. Although it is the most common cause of a vertical strabismus, the examiner should remember other causes (e.g. TED, orbital fractures) and not rush into Parks 3 step test unless the clinical picture is suggestive of CNIV palsy. Care should be taken to identifying bilateral CNIV palsies and signs indicating a congenital (versus traumatic) aetiology.
Children
Congenital: abnormal head position
Adults
Congenital: vague, intermittent vertical diplopia
Acquired
History of trauma, torsional diplopia
Bilateral
Often complain of difficulty reading (not diplopia)
1. Visual Acuity (Best Corrected)
2. Spectacles
- BD prism on affected side?
3. Inspection
- Abnormal head position- head turn / tilt to the opposite side and down
- This counters the loss of depression / intorsion. (cf. DVD where tilt is to the higher side)
- Hirschberg (Pupil margin = 15°, Iris margin = 30°)
- (Lids normal)
- (Pupils normal)
- ± Facial asymmetry (congenital CNIV) – hypoplasia on side of head turn suggests congenital
4. Cover-Testing
- Hypertropia on affected side
Parks 3-Step Test
- Does not apply if multiple muscles are involved or if there is a restrictive process i.e. do not start doing this on someone who clearly has thyroid eye disease even if there is height in primary
- This test is less useful with time due to spread of comitance
(RRR: Right hypertropia worse on Right head turn and Right head tilt; LLL).
- Determine which eye is hypertropic in primary
- Determine if hypertropia is worse with R or L head turn (worse on ipsilateral head turn due to unopposed ipsilateral IO)
- Determine if hypertropia is worse with R or L (Bielschowsky) head tilt (worse on ipsilateral head tilt due to unopposed ipsilateral SR overaction- the only intorter left)
- ± 4th step: Hypertropia worse in downgaze (chin up)? (c.f. skew deviation where it is worse in upgaze)
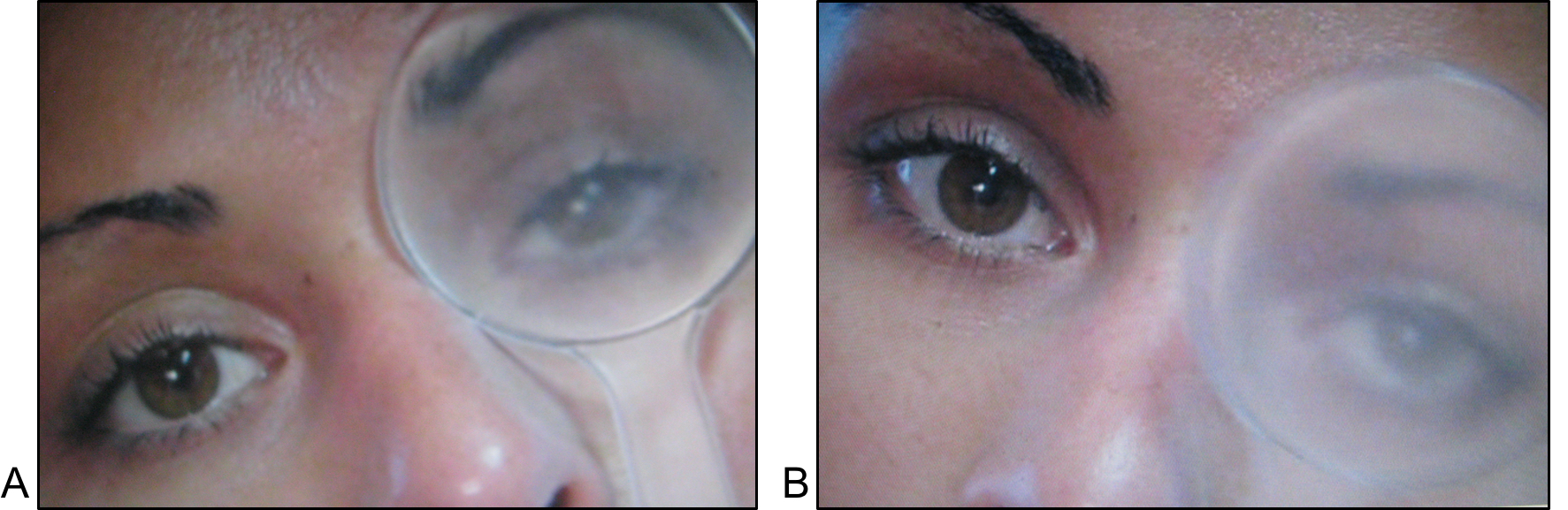
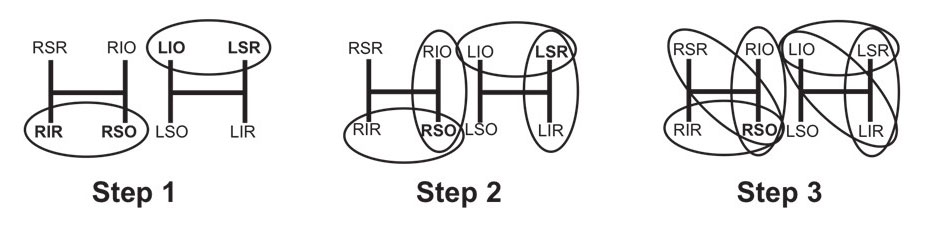
Figure 7.2.3 Parks-Bielschowsky Three-Step Test
1. Right hypertropia can be due to weakness of the right depressors or left elevators
2. Right hypertropia that increases on right head turn isolates the pathology to the right superior oblique or left superior rectus
3. Right hypertropia that increases on right head turn and right head tilt isolates the pathology to the right superior oblique
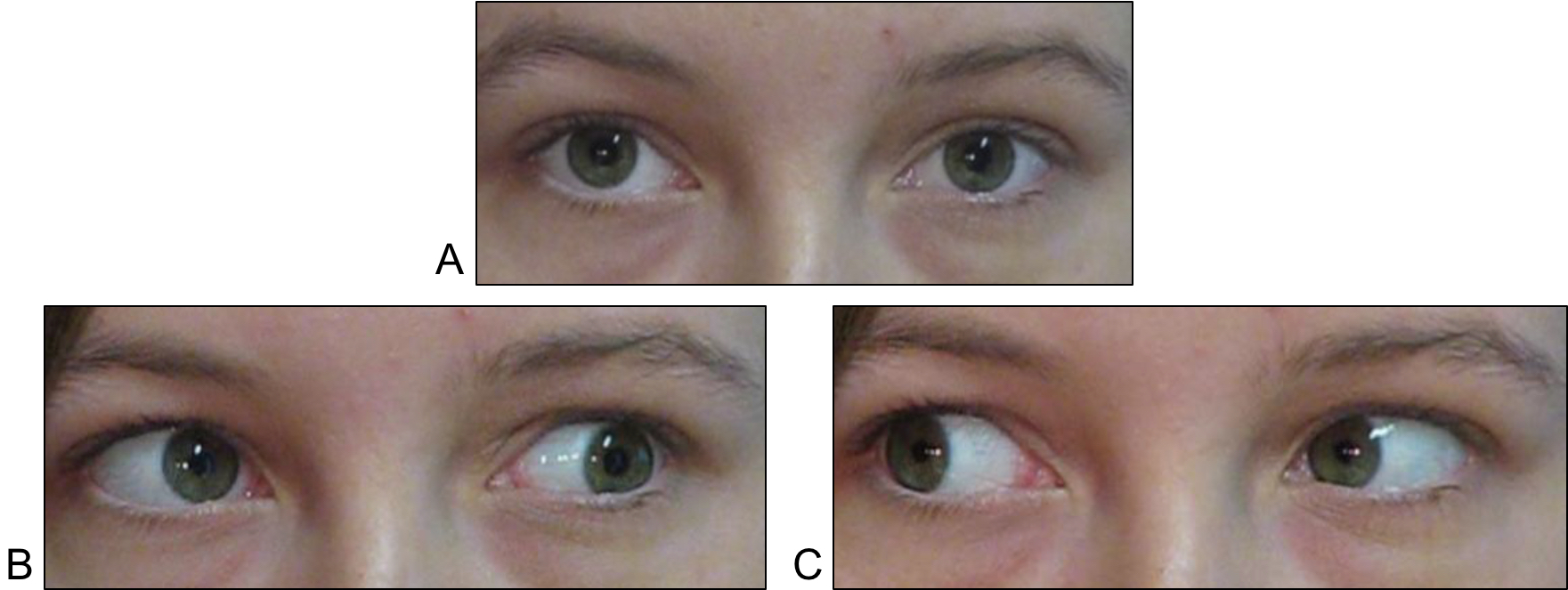
5. Ocular Rotations
Look for a “falling eye”:
- When the affected eye is fixating and adducts along horizontal, the other eye “falls”
- “IO overaction”(IOOA) & SO underaction (try chin up if can’t hold lids for alternate cover)
- Look for vertical movement on alternate cover testing
- May not be seen due to spread of comitance
6. Other Cranial Nerves
- CN III, V (corneal sensation), VII, VIII
7. Other Measurements
i. Vertical Fusional Amplitude
- Congenital CNIV >3Δ vertical fusional amplitude
ii. Torsion
- Double Maddox rod, Maddox wing, Torsion meter, Synoptophore
iii. Height
- BD prism on affected side - hold prism parallel to axis of face if there is a head tilt- i.e. not vertical
8. Fundoscopy
- Check fundus to see if fovea is (abnormally) above the optic disc (loss of SO intorsion)
Bilateral CNIV
Traumatic CNIV are often bilateral
- Chin down → diplopia worst in downgaze
- Alternating hypertropia (hypertropia of RE with R head turn, hypertropia of LE with L head turn)
- V pattern due to paralysis of SO abduction in depression
- Bilateral SO underaction, IOOA
10° of excyclotorsion on Double Maddox rod (NB: Skew deviation gives incyclotorsion)
Clinical Sign
Unilateral
Bilateral
SO Underaction (SO UA)
Unilateral
Ipsilateral SO UA
Bilateral
Bilateral SO UA
IO Overaction (IO OA)
Unilateral
Ipsilateral IO OA
Bilateral
Bilateral IO OA
V Pattern
Unilateral
<10 PD (eso)
Bilateral
>10 PD (eso)
Hypertropia
Unilateral
>5 PD
Bilateral
<5 PD (except asymmetric paresis)
Head Tilt Test
Unilateral
Increasing hypertropia on ipsilateral head tilt
Bilateral
Positive head tilt test to both sides (right hypertropia on right tilt and left hypertropia on left tilt)
Reversing hypertropia on R and L gaze
Objective Torsion on Fundus
Unilateral
Ipsilateral
Bilateral
Bilateral
Extorsion on Double Maddox Rod
Unilateral
<10 degrees (congenital usually do not have subjective extorsion)
Bilateral
>10 degrees (congenital usually do not have subjective extorsion)
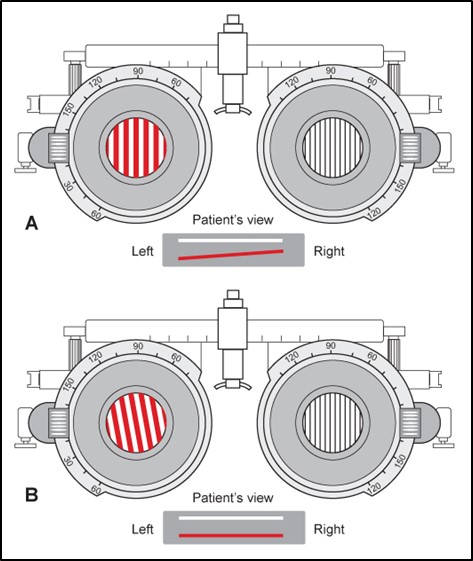
Figure 7.2.5 Double Maddox Rod Test
Maddox rods are placed vertically in front of each eye. In a CNIV palsy the (horizontal) line image of one will not be parallel to the other because of excyclotorsion of the eye. The amount of excyclotorsion can be measured by rotating the lens until the images of the two lines are parallel. In a bilateral CNIV palsy the amount of excyclotorsion is typically >10°.
Congenital CNIV
Usually unilateral with decompensation.
Usually an abnormal tendon:
- Usually less symptomatic torsion / diplopia, despite objective torsion
- Old photos (head tilt)
- Facial asymmetry (“apex” to opposite side in majority)
3Δ vertical fusional amplitude (however, fusional amplitudes are also increased in long-standing acquired deviations e.g. TED)
Summary
- Right or left (unilateral or bilateral)
- Isolated or other associated CN palsies
- Congenital
1. Congenital
2. Trauma (Often Bilateral)
Uncommonly
3. Vascular
4. Neoplastic
5. Inflammatory
6. Infective
- ± MRI brain
- Other CN palsies
- Progressive
- BP, BSL / HbA1C, Lipids (for vascular risk factors)
- ± ESR / CRP (for GCA)
- ± Tests for Myasthenia
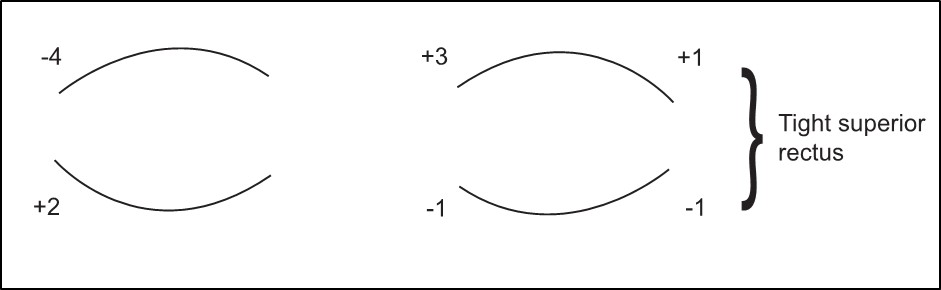
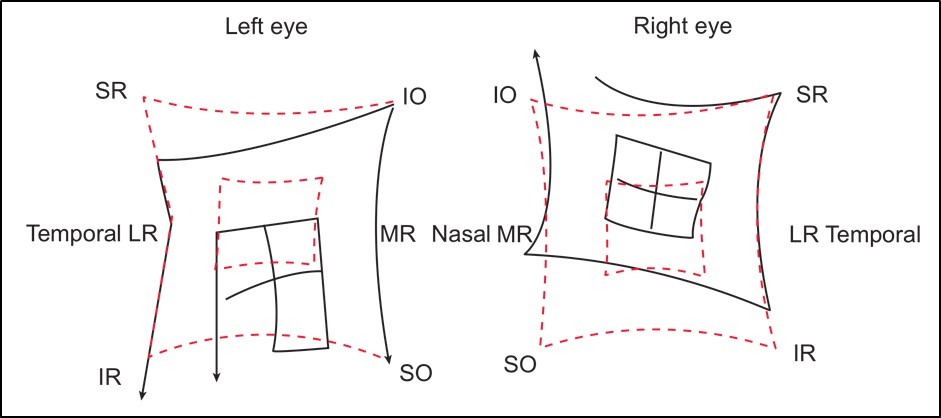
- Hess (right CNIV palsy)
- No difference in chart size
- R hypertropia especially on adduction
- R chart: Underaction of SO, Overaction of IO
- L chart: Overaction of IR, Underaction of SR
- Look at old photographs – driver licence
NB: Remember that a Hess chart does not measure torsion.
Indications for Treatment:
- Abnormal head posture
- Diplopia
- (Cosmesis)
- Uniocular occlusion for diplopia
- (Fresnel) Prism (BD on affected side) if there is minimal torsional component
- Only have to prescribe enough for comfort (not necessarily the whole amount up to 10Δ is reasonable)
All rights reserved. No part of this publication which includes all images and diagrams may be reproduced, distributed, or transmitted in any form or by any means, including photocopying, recording, or other electronic or mechanical methods, without the prior written permission of the authors, except in the case of brief quotations embodied in critical reviews and certain other noncommercial uses permitted by copyright law.

Vitreoretinal Surgery Online
This open-source textbook provides step-by-step instructions for the full spectrum of vitreoretinal surgical procedures. An international collaboration from over 90 authors worldwide, this text is rich in high quality videos and illustrations.